Gritty sensation in the eyes, persistent redness, sensitivity to light, and slightly impaired vision.
Many people may feel anxious when these symptoms persist.
Symptoms that you might have thought were a stye or conjunctivitis could actually be a viral infection called “ocular herpes.”
The most crucial aspect of treating ocular herpes is accurately determining whether “the virus is actively replicating” or if “the body’s immune response is overactive.” This distinction is vital because the appropriate medications differ completely based on this assessment.
This article will systematically explain what ocular herpes is, why it occurs, and what types and treatments are available.
The “Latent Virus” that many People Carry without Knowing
Ocular herpes is caused by the Herpes Simplex Virus (HSV) or the Varicella-Zoster Virus (VZV), which causes chickenpox and shingles [2].
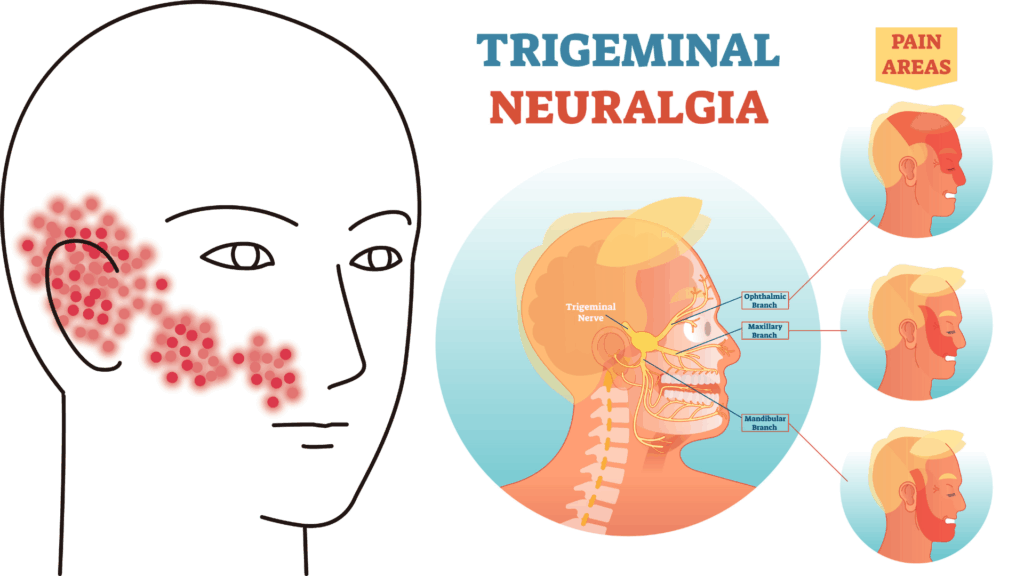
Once these viruses infect the body, they don’t completely disappear. They remain dormant in the ganglia at the base of the trigeminal nerve, which transmits facial sensations to the brain (latent infection) [2]. It’s similar to an animal in hibernation.
While usually causing no symptoms, triggers such as fever, physical and mental stress, UV radiation, or weakened immunity can cause the virus to reactivate [5]. The dormant virus awakens, travels along the nerves to reach the eye’s surface and interior, causing various symptoms.
In developed countries, corneal diseases caused by herpes simplex is one of the leading causes of infectious blindness [2].
Eye Diseases Caused by Herpes Simplex Virus (HSV)
The herpes simplex virus affects various parts of the eye, including the eyelids, conjunctiva, cornea, iris (the colored part of the eye), and retina. Corneal diseases are particularly common.
When inflammation occurs in the iris, it’s called herpetic iritis (uveitis).

Corneal Herpes: Two Types with Different Treatment Approaches
Corneal herpes is broadly classified into two types based on how the disease develops, and their treatments are completely different.
1. Type Where the Virus Directly Affects the Cornea (Epithelial Keratitis)
This occurs when the virus actively multiplies in the “epithelium,” the outermost layer of the cornea [8].
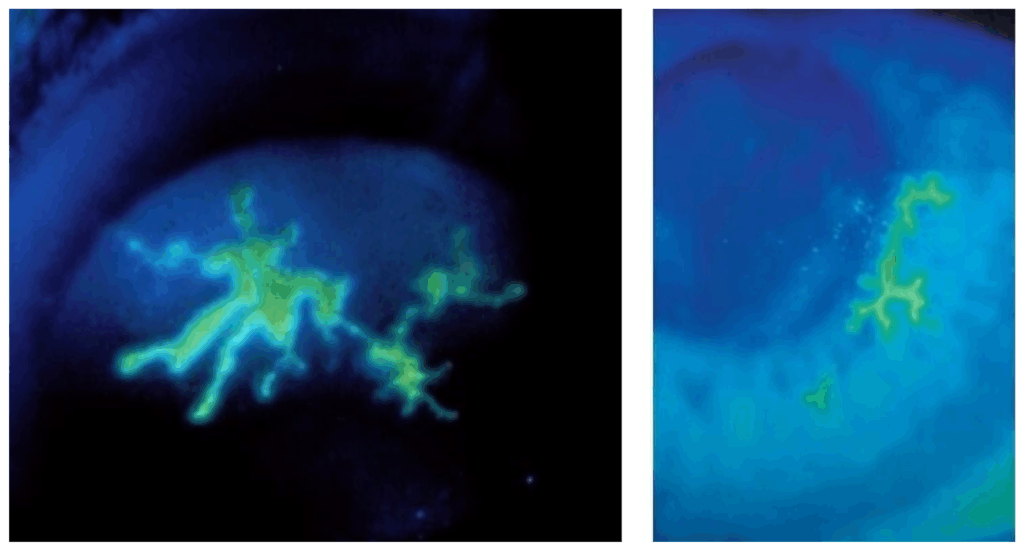
A characteristic feature is the “dendritic ulcer,” which resembles tree branches or lightning patterns. Eye doctors can diagnose this using special staining and microscopy [8]. These lesions form as the virus multiplies and destroys cells. Common symptoms include pain, foreign body sensation, redness, tearing, and light sensitivity.
The primary treatment for this type is antiviral medication that directly suppresses viral replication, mainly in the form of eye drops or ointments [8]. However, caution is needed as using steroid medications at this stage to reduce inflammation can promote viral replication and worsen the condition.
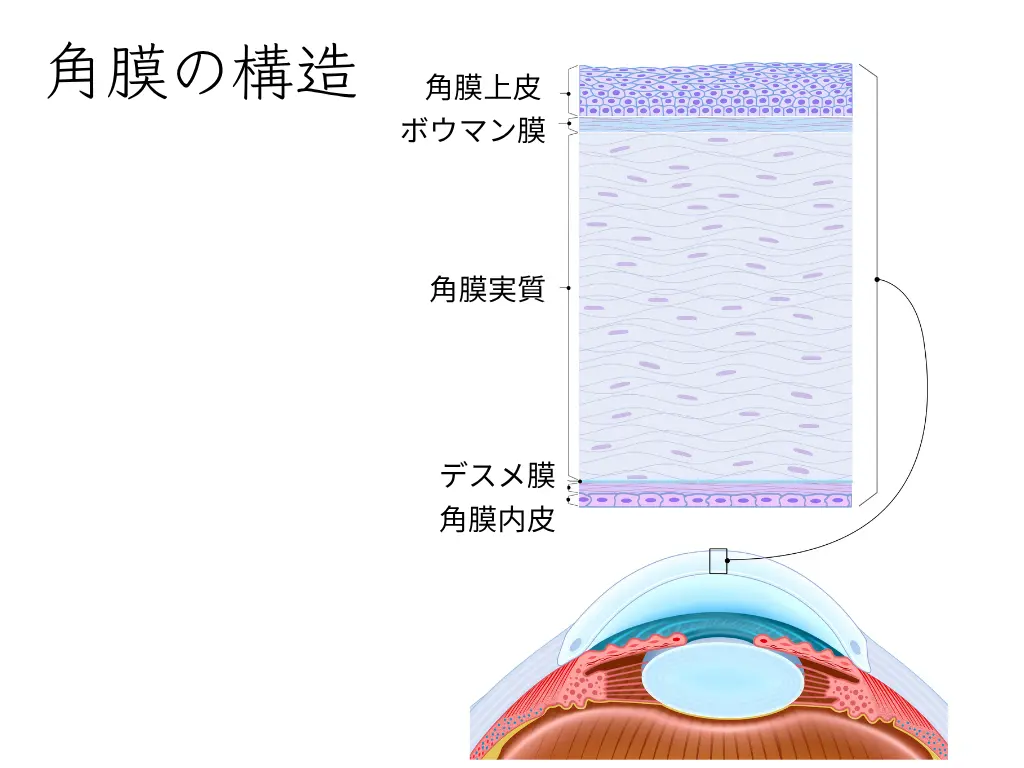
2. Type Caused by the Body’s Immune Response (Stromal Keratitis)
This type involves inflammation in the deeper “stromal” layer of the cornea.
Rather than viral replication itself, this occurs when the immune system overreacts to viral fragments remaining in the cornea [2].
It’s like the body’s defense mechanism “attacking friend instead of foe,” damaging its own corneal tissue despite trying to help.
Main symptoms include blurred vision and reduced visual acuity, with relatively mild pain in some cases.
The main treatment here is steroid medication to suppress the excessive immune response.
However, using steroids alone can cause dormant viruses to reactivate, so antiviral medications are used in combination [6].
This treatment approach was established through the large-scale clinical research known as the Herpetic Eye Disease Study (HEDS) [6, 7].
Thus, even within corneal herpes, the treatment approach differs significantly depending on whether the main cause is “viral activity” or “immune response.”
Herpes Simplex beyond the Cornea
Herpes simplex can cause inflammation in areas beyond the cornea.
Corneal Endotheliitis
When endothelial cells in the innermost layer of the cornea are damaged, the entire cornea swells, leading to decreased vision [2].
Iridocyclitis (Uveitis)
Inflammation occurs in the iris (the colored part of the eye) and the ciliary body behind it, which controls focusing. This causes blurred vision, eye pain, and redness. Eye pressure can rise suddenly [2].
In these conditions too, the body’s immune response is the main cause, so treatment typically combines steroid and antiviral medications.
Eye Diseases Caused by Varicella-Zoster Virus (VZV)
When shingles on the face involves eye symptoms, it’s called Herpes Zoster Ophthalmicus (HZO).
This occurs when the same virus that causes chickenpox reactivates in the first branch of the trigeminal nerve, which covers the area from the forehead to the eye and nose [4].
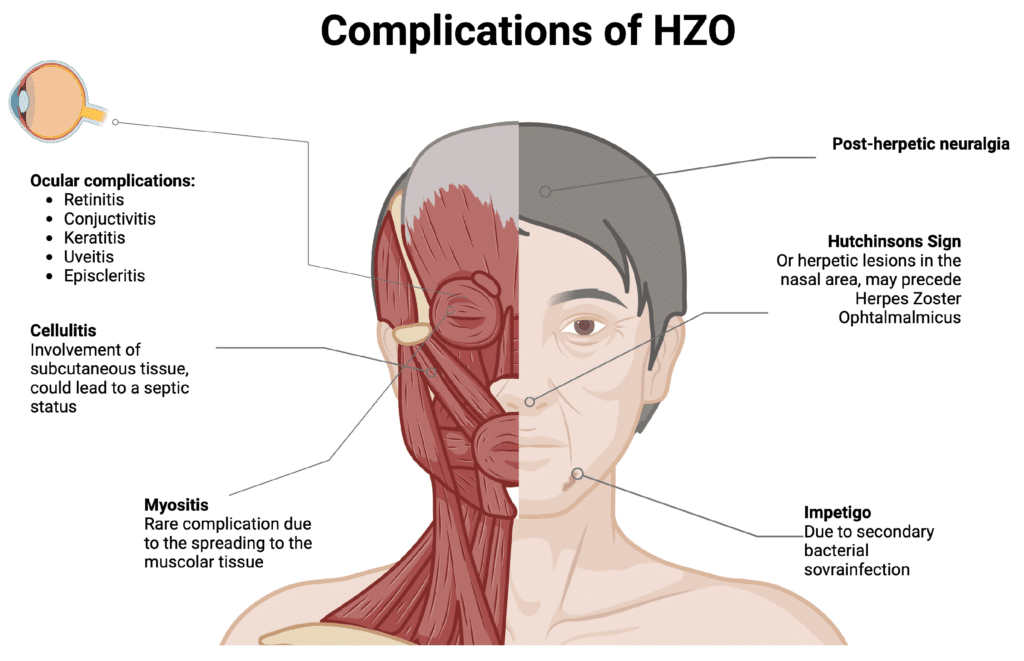
Nasal Rash as a Danger Sign: “Hutchinson’s Sign”
Special attention is needed if rashes appear on the tip or side of the nose along with forehead rashes.
This is called “Hutchinson’s sign” and indicates a very high risk of ocular complications [4].
This is because the tip of the nose and the eye are innervated by the same nerve (nasociliary nerve).
If you notice this sign, seek immediate ophthalmological care.
Various Eye Complications and Sequelae
Herpes zoster ophthalmicus can cause conjunctivitis, keratitis, uveitis, and increased eye pressure [4].
Additionally, nerve damage from the virus can lead to long-lasting nerve pain (Postherpetic Neuralgia, PHN) even after treatment [4].
The most crucial aspect of treatment is starting high-dose antiviral medication within 72 hours of rash onset. Early treatment has been shown to significantly reduce the risk of eye complications and sequelae [1].
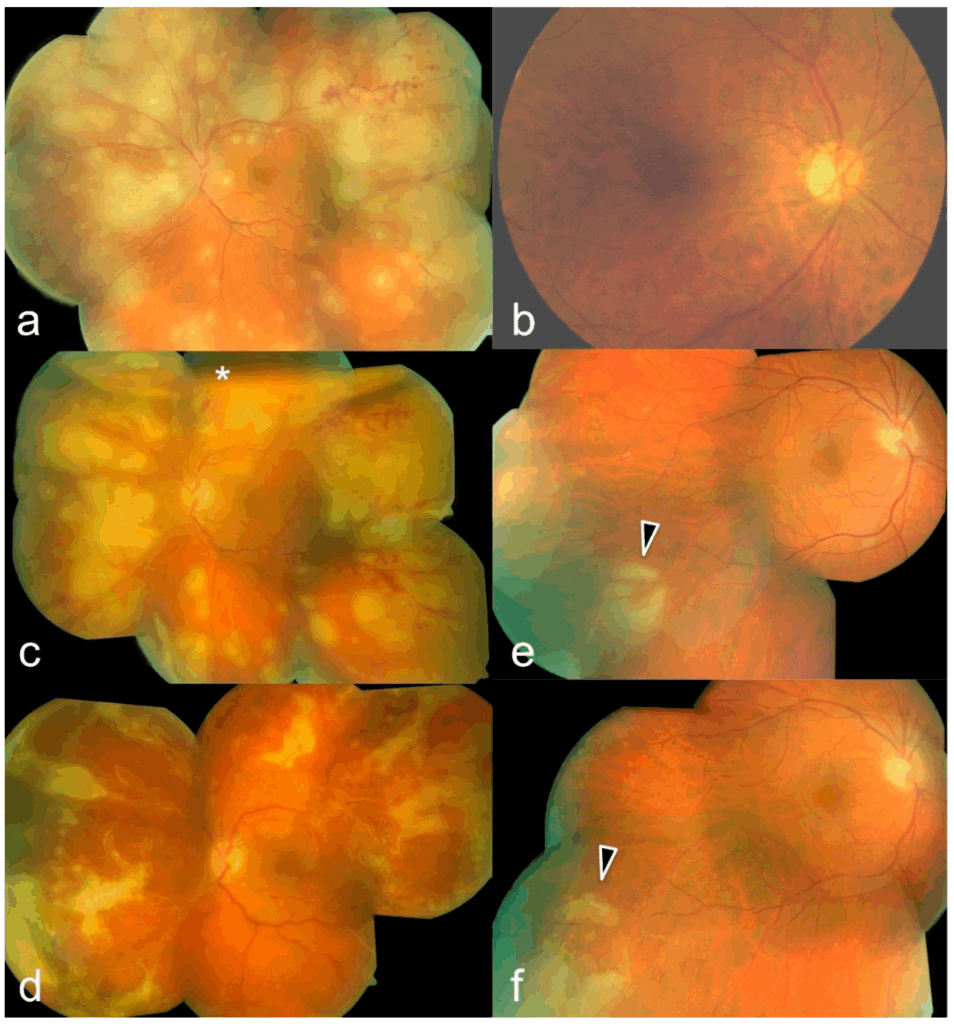
Critical Warning Signs: Retinal Herpes
Though very rare, herpes virus can infect the retina, causing a serious condition called Acute Retinal Necrosis (ARN) [5].
This is an ophthalmological emergency that progresses rapidly and can lead to blindness due to extensive retinal destruction [5].
If you experience sudden vision loss or visual field defects, seek immediate care at a specialized medical facility.
Treatment involves intensive care, including intravenous antiviral medications and intraocular injections [5].
Even mild initial inflammation often begins in the peripheral retina.
Therefore, it’s important for ophthalmologists to examine the peripheral retina.
Modern ultra-wide-field fundus imaging now allows for peripheral screening.
Preventing Recurrence
Ocular herpes tends to recur even after complete recovery. Preventive treatment is particularly important for patients who experience repeated stromal keratitis, which significantly affects vision.
Long-term Preventive Medication
The HEDS study proved that taking low-dose antiviral medication daily for over a year reduces the recurrence rate of all types of ocular herpes by about 40% and stromal keratitis by about 50% [7].
Prevention before Eye Surgery
Eye surgeries like cataract surgery or corneal transplantation can trigger dormant herpes virus reactivation [2]. For patients with a history of ocular herpes, preventive antiviral medication before and after surgery is highly effective in preventing recurrence.
Shingles Vaccine
A highly effective vaccine (Shingrix®) is available for people aged 50 and older to prevent shingles [3]. This vaccine helps prevent not only shingles itself but also complications like herpes zoster ophthalmicus and postherpetic neuralgia [3].
Summary
While ocular herpes is a single disease, its symptoms are highly diverse. It ranges from conditions where actively replicating virus is the problem to those caused by the body’s immune response.
- For epithelial keratitis, antiviral medications are the primary treatment.
- For stromal keratitis and uveitis, careful use of steroid medications with supportive antiviral medication is key to treatment.
- For herpes zoster ophthalmicus, starting oral antiviral medication as early as possible is particularly important.
For any type, it’s dangerous to self-treat with over-the-counter eye drops or discontinue treatment.
If you have persistent eye symptoms, don’t “wait and see” – seek prompt care from an eye specialist. Early detection and treatment is the best way to protect your precious vision.
References
- Balfour, H. H., Jr, Bean, B., Laskin, O. L., Ambinder, R. F., Meyers, J. D., Wade, J. C., Zaia, J. A., Aeppli, D., Kirk, L. E., Segreti, A. C., & Keeney, R. E. (1983). Acyclovir halts progression of herpes zoster in immunocompromised patients. The New England journal of medicine, 308(24), 1448–1453. https://doi.org/10.1056/NEJM198306163082404
- Farooq, A. V., & Shukla, D. (2012). Herpes simplex epithelial and stromal keratitis: an epidemiologic update. Survey of ophthalmology, 57(5), 448–462. https://doi.org/10.1016/j.survophthal.2012.01.005
- Lal, H., Cunningham, A. L., Godeaux, O., Chlibek, R., Diez-Domingo, J., Hwang, S. J., Levin, M. J., McElhaney, J. E., Poder, A., Puig-Barberà, J., Vesikari, T., Watanabe, D., Weckx, L., Zahaf, T., Heineman, T. C., & ZOE-50 Study Group (2015). Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults. The New England journal of medicine, 372(22), 2087–2096. https://doi.org/10.1056/NEJMoa1501184
- Sanjay, S., Huang, P., & Lavanya, R. (2011). Herpes zoster ophthalmicus. Current treatment options in neurology, 13(1), 79–91. https://doi.org/10.1007/s11940-010-0098-1
- Schoenberger, S. D., Kim, S. J., Thorne, J. E., Mruthyunjaya, P., Yeh, S., Bakri, S. J., & Ehlers, J. P. (2017). Diagnosis and Treatment of Acute Retinal Necrosis: A Report by the American Academy of Ophthalmology. Ophthalmology, 124(3), 382–392. https://doi.org/10.1016/j.ophtha.2016.11.007
- Barron, B. A., Gee, L., Hauck, W. W., Kurinij, N., Dawson, C. R., Jones, D. B., Wilhelmus, K. R., Kaufman, H. E., Sugar, J., & Hyndiuk, R. A. (1994). Herpetic Eye Disease Study. A controlled trial of oral acyclovir for herpes simplex stromal keratitis. Ophthalmology, 101(12), 1871–1882. https://doi.org/10.1016/s0161-6420(13)31155-5
- Acyclovir for the prevention of recurrent herpes simplex virus eye disease. Herpetic Eye Disease Study Group. (1998). The New England journal of medicine, 339(5), 300–306. https://doi.org/10.1056/NEJM199807303390503
- Wilhelmus K. R. (2015). Antiviral treatment and other therapeutic interventions for herpes simplex virus epithelial keratitis. The Cochrane database of systematic reviews, 1(1), CD002898. https://doi.org/10.1002/14651858.CD002898.pub5